


New Safe Harbor “Wellness Programs” Being Instituted by State Legislatures To Protect Physicians in Getting Help (FULL-LENGTH Version)(see below for PODCAST link)
Are These "Wellness Programs" Moving In on PHPs’ Territory To Offer Safe Access To Psychologically-oriented Help? And … Are They Safe? Mmmm... Yes, and Maybe Not.

(Truth be told, this is not so much a blog post as it is a short-length novel. Since not everyone wants to read long-form journalism with Proustian-length sentences, no matter how erudite or witty, I offer a shorter version here. Same essential stew but without the spices, and a lot less heat.)
And, here’s the accompanying podcast.
PODCAST of this article: (https://physicianinterrupted.substack.com/p/podcast-to-accompany-new-safe-harbor)
I’m still exploring the Substack capabilities, so please pardon the redundant messages if they’ve occurred.
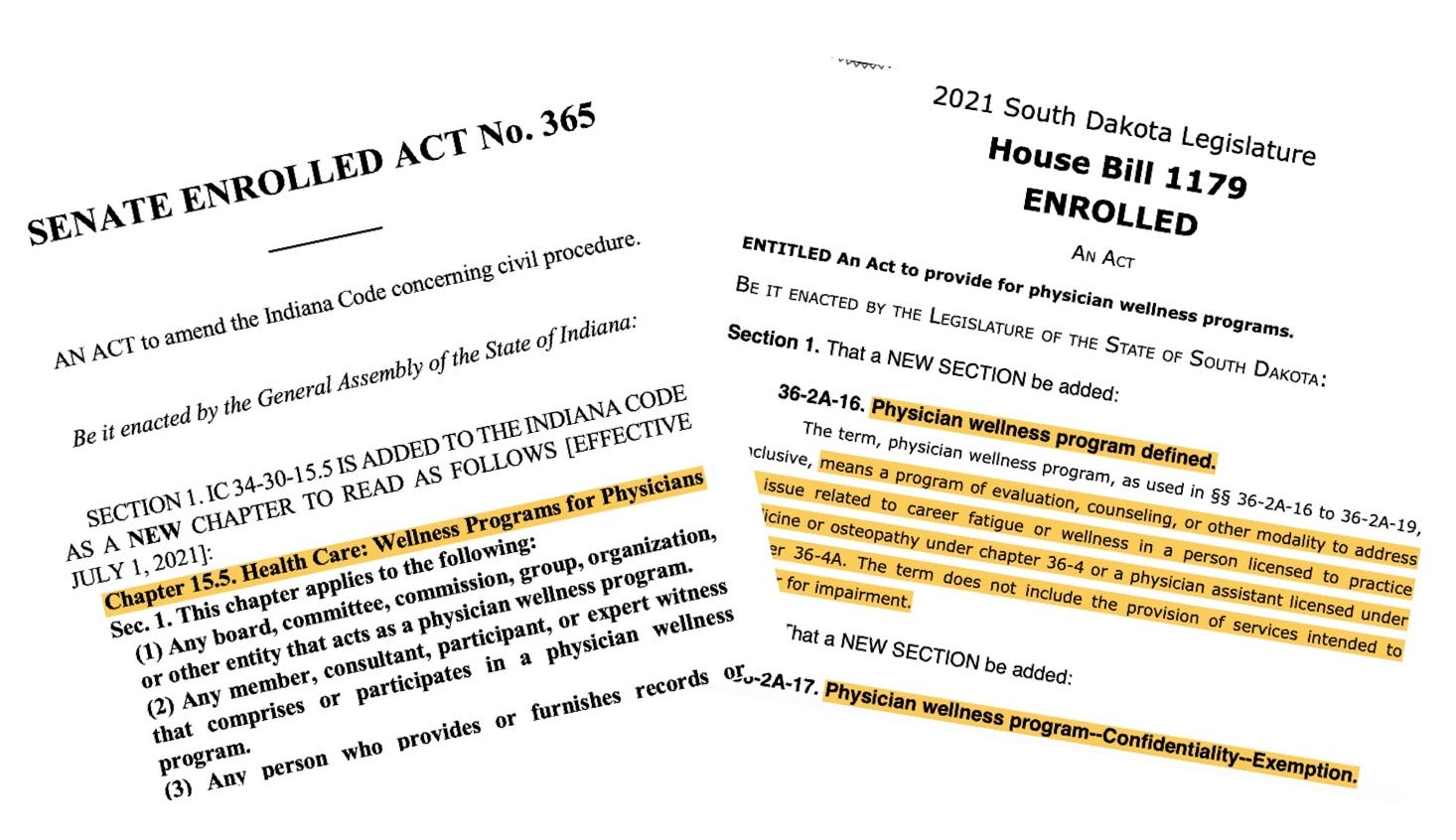
A coaching colleague just shared a recent blog post from HappyMD’s Dike Drummond pertaining to recent bills and enacted laws in three states, manifestly designed to protect the confidentiality of physicians seeking help for psychologically oriented “wellness services” in the context of their professional lives. (You may have thought that your confidentiality was already protected. Alas, to paraphrase one PHP director, you would have been mistaken.)
I’m glad that Dike has shared these developments. He seems enthusiastic and hopeful that this will remedy physicians’ reluctance to get help.
While on the surface there appears to be cause to be reservedly enthusiastic and hopeful, I’ve got numerous - and growing - reservations. I still see significant danger for physicians who seek any such services from these newly-minted wellness programs, especially if they’re operated by any party affiliated in any way with boards or PHPs. I maintain grave concerns about the ever-evasive, chameleon-like identity of PHPs and their boundaryless fluidity with boards (MLBs).
Of the three states, South Dakota’s and Indiana’s appear most straightforward and indeed secure.
Virginia’s remains obscure despite my reading it several times. And so I can’t give it a thumbs up, because I can’t make head or tails of it. Which, by the way, is one of the problems with this sort of legislation. If you, a reasonably intelligent professional, can’t make sense of it, you can be certain of one thing: you don’t have a solid footing to protect your rights.1 Perhaps someone could offer in the comments a concise translation of Virginia’s lego-speak and what the law really says.
See this footnote for some abbreviations you’ll see throughout.2
The Newly Legislated “Wellness Programs”
First, the good news. Why I believe these bills/laws (at least two of the three) are helpful. It’s not per se in what they propose as much as in what they signify.
They demonstrate legislators’ genuine concern about physicians’ not being able to safely get psychological help without being pulled into the board’s and PHP’s crazy-making universe and being driven to either suicide or bankruptcy and a psychically broken life of morally assaulted despondency.
Clearly, these initiatives are being brought forth in part by some who are genuinely concerned about physician wellbeing. For that, and especially those who are active in pushing forward legislative initiatives that serve to genuinely help physicians while also protecting their rights, I think we all owe our appreciation. A lot of social justice legislative advocacy work like this goes on unseen. These legislative efforts give formal recognition that docs as a whole are in trouble with burnout, the cumulative toll of trauma and PTSD, and deep moral injury. And they need exquisitely skillful help that is focused, effective, readily available, and air-tight fail-safe to obtain.
But … are these “wellness” services?
Well, if you call a medic’s stemming a life-threatening hemorrhage of a soldier’s traumatic injury a “wellness service,” okay.
So, in a very indirect, non-accusatory way, these new laws recognize that getting help through a PHP may be dangerous for physicians’ careers and their personal wellbeing. But from my perspective, (and, disclaimer, I have not read the deliberations behind these bills,) each of these bills tiptoes around the predatory culprits which have made safely getting help impossible.
Nevertheless, and most importantly, these legislators recognize that the help physicians need must be safe and protected from incurring any harm from the pseudo-benevolence and the self-interested referral of exclusively contracted PHPs which feed their monstrously ravenous ASAM-predominated “impaired physician rehabilitation program” referral funnel.
They seem also to recognize that getting psychological help in any way is dangerous as, if you have to report it to an entity such as a board or a credentialing entity for your staff appointment and your employment, it could irreparably harm you as it could suck you into the MRTC vortex from which you have little chance of escape or career survival.3
So it’s absolutely got to be safe from medical boards’ prying eyes and their assaultive police power overreach.
My Apologies If I Offend Some.
I recognize that these critical descriptors of boards and PHPs contained in this essay are both generalizations and are very strong assertions to make. I suspect that not ALL boards and PHPs are as violative as those I’ve become familiar with through hundreds of physicians’ stories. But my harsh appraisals are based on conversations with over five hundred physicians over the past several years as executive director of CPR, The Center for Physician Rights. And alas, they concur with my own personal experience.
Barbed though it may be, I hope my critique will be seen as an invitation to straightforward dialog with concerned legislators and other leaders considering proposing such bills.
Should any legislator, board or PHP leader, or any medical leader wish to have an open discussion, perhaps as a group of us via an interactive webinar, I would welcome hosting such or participating as a guest. I think such frank point-counterpoint dialog would benefit all of us. Despite recently being publicly portrayed by one medical board in an international presentation as a dangerously mentally ill physician who deserves only ridicule as a noxious insect and whose opinions, apparently especially those critical of boards and PHPs and their national associations, should be disregarded as meaningless psychotic babbling, I promise I can hold it together and make myself sufficiently presentable.4
Why These Wellness Program Bills/Laws May Be Inadequate … If Not Dangerous.
First, they generally legitimize PHPs as the widely accepted deliverer of both physician impairment – and now of psychological wellness – services. And there’s no basis in fact for affirming either, except for PHPs’ relentless self-affirmations that they are the definitive go-to authority. Sorry to differ. They aren’t. In a significant number of cases, they’re a bunch of recovering drunks and druggies, some who’ve relapsed numerous times, who’ve had their records expunged through “connections” but who mete out medicalized punishment like brainwashed Stockholm syndrome detainees.
By legislators giving such tacit approval, they unwittingly feed docs into a dangerous PHP system with its “preferred relationships” that more resembles a self-interested referral scheme if not a RICO, and perpetuates its lack of definitional and thus legal-delimiting boundaries. They don’t recognize PHPs’ inherent lack of independence from MLBs. And they still make no effort to hold PHPs and MLBs accountable for their past denial of rights. These key concerns are detailed below.
No Accounting For Past Harms
I recognize that the purpose of these bills is sincerely well-meaning (well, at least it appears that way) to afford the safe operation of a “physician wellness” program. But these bills still indirectly give deference to PHPs as the wellness program deliverers.
But many contend that it is these very physician health programs perpetuated the harms that drove the production of these new “safe harbor wellness program” laws. These bills/laws do not account for past harms by these invasive boards and PHPs which have craftily punished – via “medicalization,” indeed “extraordinary rendition” – physicians who have sought help, many in contexts that were entirely outside of any patient complaint or quality of practice concern.
To me, ignoring these harms is like telling Jack the Ripper that he can continue to date as long as we don’t hear another peep (or scream).
In NC, the state auditor essentially stated in 2014 that NCPHP had violated the due process rights of all 1,140 physicians it psychiatrically assessed under its coy “peer review” camouflage identity over the preceding decade. Neither NCPHP nor NCMB nor any component of state government including the Governor, the Attorney General, or the State Auditor did anything to investigate this systematized wrongdoing or to mitigate its harms.
1,140 physicians.
Denied requisite due process.
Via deceptive practice of a purported state agency.
Denying each and every one of them their fundamental rights.
One can speculate as to why that might be the case. Gargantuan potential financial liability for one. Nastily unattractive inernational visibility for another. Who’d want to practice in a state where physicians’ rights and their very careers could so recklessly be assaulted? Nice beaches and mountains, eh doc? So sorry you’re unemployed and can’t practice as a doc anymore anywhere in the world. Sure wish we had better laws but, hey, what can you do?
These “safe harbor wellness program” laws allow PHPs to remain ill-defined in their medico-legal identity and accountability. Doing so gives them continued opportunity to do harm that will still go unpunished and allow them to continue to feed their “preferred” network.
In short, there has been no reckoning of the harms done - they’ve all been swept under the rug.
The Elusive Chameleon Identities of PHPs
PHPs operate as chameleons under diverse and continuously changing deceptive identities that then become ensconced in state law and give them protection. Witness this sampling: “peer review;” “case manager;” “screening program;” “facilitator of referral to a ‘preferred program’” etc.
Providing help under the guise of a benevolent “trust me, I’m your friend” identity and then pouncing a surprise revelation is equivalent to an accounting agency presenting itself as a specially knowledgeable tax preparer offering to help you prepare your taxes and use all available loopholes. And then after submitting your taxes, informing you they were actually working for the IRS and what you said may be held against you. Oh, and that you’re being sent to Kansas for a four-day evaluation of your competency to ethically manage your finances and to investigate you for criminal theft and that after that, you’ll be sent to a 3 month “preferred physicians’ accounting camp” for thorough rehabilitation in your approach to tax preparation. So as to “protect society,” you’ll be monitored afterward for 5 years not only for your ethical tax preparation but for every expenditure you make, and you’ll have to report to your account parole officer for random production of all purchases and receipts. And for good measure, you’ll be attending PHP continuing ed run by group facilitators with the personality of Nurse Ratched who’ll send us reports of your improved behavior for years to come.
And if you balk at this, you’ll immediately be reported to the IRS as a criminal tax cheat and you will lose all rights to your license to make a living as a physician as, after all, your medical license is a “privilege” and not a “right,” and you shouldn’t be able to operate in such a dangerous way that threatens to harm patient safety because of your awful ethics of accounting. Who knows, you’re probably fleecing patients! After all, your irresponsible behavior besmirched the vaunted integrity of the entire medical profession.
As facetiously absurd as this analogy is, I regret to report that the reality of these career- and psyche-destroying enterprises, a disturbing number of which are staffed if not run by drug thugs who have had their records expunged but have retained their MDs, is even worse.
Given FSPHP’s aversion to open dialog (numerous invitations made) and one PHP’s persistent refusal to provide records of its operations and the laws governing it - these latest requests made in the context of its possible role in a serious PHI breach by its boundarylessly contracted board - from my perspective, there is no imaginable scenario in which a physician should ever willingly initiate going to a PHP. None.
PHPs are generally not licensed as medical corporations and yet are conducting life-altering diagnostic evaluations (or “screenings”) whose results they refuse to share with physicians but which results they freely disclose to boards which then order unquestioning compliance with whatever the PHP says, presumably including brain biopsy if they so chose. (I write this in only slight jest; visit FL laws to see what a PHP is empowered to do, non-compliance with which will essentially cast you out of medicine worldwide as a pariah to be scorned.5
PHPs Have Embraced Mission Creep
The legislators behind these safe harbor wellness initiatives are most likely completely unaware that the PHP movement has been expanding its scope of declared expertise. That it actually possesses any of the declared expertise is highly suspect.
“We Help Docs With Burnout”
The well-intentioned legislators may be completely unaware that there’s a movement afoot by PHPs to classify burnout as “depression.” So with depression as a DSM “mental illness” and all of its stigma, your newly diagnosed “depression” is now thus a “potential danger to patient safety.” So now, you’re not just burned out. You’re mentally ill – and a danger to society! (“Poor you, let us help you” they exhort, “let us show you some of our brand of compassion.”)
If you thought you were grappling with burnout before … try navigating this!
Legislators are likely ignorant of the precise language of impairment as delineated in the ADA, and the fact of its apparently willful misuse by PHPs and boards. They probably also don’t know that PHPs and their national association FSPHP, in full concert with FSMB which publishes presumably lawyer-informed guidelines on the assessment of “impaired physicians” officially promulgates a policy on impairment that is quite troubling.6 In fact, it appears to at least one prominent ADA specialist as being fundamentally in violation of numerous essential tenets of ADA.
To FSMB, there is no distinction between actual functional work impairment from a bona fide time-limited disability, a physician’s “potential for impairment,” and anyone having a medical condition that is “potentially impairing.” When simply living and practicing your profession is a risk factor for being alleged to be “potentially impaired” and thus a danger to patient safety, uh, “Houston, we have a problem.” You’ve created a program that has an endless stream of lucrative customers not to mention a veritable minefield that physicians must navigate. (Speaking of mines, it also appears to be a gold mine for that select group of lawyers self-described as specializing in “professional license defense.” For too many, it seems they’ve adopted the practice of collecting $10K or $20K upfront, writing a few showy letters and then telling the doc they’ve got to do what the board says.) It’s an ideal inter-referral scheme for everybody … everybody that is except the accused doc.
But Wait! PHPs Were Already Supposed To Be Safe Harbors
Legislators are likely unaware that PHPs have already deceptively portrayed themselves as safe harbors. And yet, even now, we see them eagerly offering to help physicians with their burnout plight while at the same time elsewhere arguing that burnout is in itself a “potentially impairing condition” that could lead to depression and to diminished patient outcomes. And such is therefore a “safety issue” and “our job is to protect patient safety” (it is not in fact their primary mission – yet another deception) and could warrant their emergency intervention and their abruptly “breaking confidence” and give full cover to their contracted board (the one that pays their salary to keep their racket going) to immediately yank that physician’s license.
“If you weren’t impaired comrade, why would they send you to us ?”
So everyone who walks through the PHP door is by definition potentially “impaired.” Otherwise, in true Kafkaesque fashion, they reason, “why would you be sent, comrade?” And since “potentially impaired” = “danger to society,” the outcome is “go along with us, doc, or we’ll have to release the monkeys, and you know what happens then, don’t you? They’ll do their emergency powers routine and threaten to declare you as a menace to all of mankind if you don’t go along. Don’t make us do that. Besides, doc, don’t you value your career? After all the time and effort and money you’ve put in, this is such a small price to pay.”7
Once ensnared, no matter how warrantless or mistaken, that physician’s career is over. And due to boards’ and PHPs’ wall of immunity, maintained somehow with utterly no governmental oversight, neither justice nor monetary recovery is available. You’ll be hard-pressed even to find a sufficiently expert lawyer conversant in this area. The bottom line here is, once pulled into their twilight zone, your career, your life as you once knew it, is over.
And … there will be no - NO - intervention by the state because the state has chosen not to see either its board or its contracted PHP as a possible manipulative wrongdoer capitalizing on its immune status. The state seems to reason “It’s much easier to let them ‘discipline their own’ and step back. Because surely, no one wants an ‘impaired physician.’ So let them do whatever they need to do.”
Even further, very few legislators - indeed even physician leaders - would know that PHPs are striving to designate the very occupation of “physician” itself as a federally designated “safety-sensitive” occupation and thus expand their authority and self-serving referral system and establish their ensconcement as the definitive impairment deciders.8 Talk about $Ka-ching$!
Laws Protecting The Privacy Of “Wellness Programs” Already Exist.
These new laws seemingly fail to acknowlege that PHPs were already defined as some variant of a “wellness program” (after all, what else does the term “physician health” connote?). Some specifically identify themselves as subject to the strictest federal confidentiality provisions - those of 42 CFR Part 2; they were already subject to federal and state privacy laws. But operating under the protection of the contracting MLB and enjoying that MLB’s extension of state immunity (or at least giving the appearance of same to the courts), they giddily operate in an environment safe from suit.
And, as seen in the NC 2014 audit of NCPHP which determined that for all intents and purposes, NCPHP had systematically violated the due process rights of 1,140 physicians it had “peer review” psychiatrically evaluated over the preceding decade, law – whether passed by the state legislature or enacted by Congress – means nothing to them. With a non-overseen program deceptively operating as a peer review entity with completely risk-free immunity, you can get away with just about anything, including career homicide.
The Beguiling Apparition Of Law-Guaranteed Privacy
Wellness programs are generally covered under various provisions of law as to their obligation to maintain confidentiality and, if employer-sponsored, to have separate record-keeping, esp. insofar as acquiring any PHI from participants.
Despite intensive study over the past six months of HIPAA, HITECH, 42 CFR Part 2, ADA, diverse state privacy laws, federal laws governing the medical evaluation of employees et al., I still remain uncertain about what laws apply to a PHP – in large part because of their evasive chameleon-like identity. Now, with its or some other entity’s designation as a “wellness program,” does it have obligation to ensure the privacy of PHI under HIPAA and any other federal laws ? These three Wellness Program laws are state laws that, if stricter than federal PHI privacy laws, should prevail. But one does need to ask, why didn’t existing federal laws such as HIPAA, 42 CFR Part 2, and ADA to name but three suffice to protect confidentiality? Why didn’t professional psychological guidelines pertaining to ethical duties of confidentiality and to ethical fitness for duty exams, and laws prohibiting involuntary commitment and group practice of medicine without a license and deceptive practice under false pretense work?9
It’s vital to examine these questions as, left unexamined and simply superimposing new laws, what’s to say these too won’t be ignored?
It would seem apparent that MLBs, as designated HIPAA “health oversight” agencies, are subject to its privacy and security provisions. Yet one may find it difficult to get a straightforward answer to their HIPAA responsibilities; my repeated requests to NCMB and NCPHP for clarification have gone unanswered. I’d encourage you to ask - in writing - whether your MLB is a “health oversight” entity under HIPAA and is subject to HIPAA’s privacy and security provisions. Ask your state’s PHP are their evaluations of physicians diagnostic in nature? Are they covered under HIPAA? Are they covered under 42 CFR Part 2? Are they subject to ADA? Do they carry malpractice insurance? Who oversees them? What is their policy if a physician feels they’ve been wrongfully “screened” or wrongfully evaluated by a “preferred” program? Be prepared for a long period of non-responsive silence.
And it would seem that PHPs surely would be subject to HIPAA and perhaps to 42 CFR Part 2 which strictly protects the confidentiality of all who have entered a federally assisted alcohol and drug assessment and treatment program, even involuntarily, and even if only for assessment. But they evade this by claiming that the diagnostic or screening evaluation they conducted wasn’t really such, despite the fact that the MLB and thus the state and the courts consider them as having been definitively diagnostic and so awesome and unchallengeable in their scientific truthfulness as if the Creator had infallibly declared such.
Without Enforcement And Penalty And Right Of Private Action, All This “Safe Harbor” Talk Is Just Illusory
But as I learned from one public advocacy lawyer, even with laws “on the books” protecting such privacy, getting federal or state enforcement of that law is wishful thinking. And further, finding affordable legal representation should your privacy rights have been violated is another thing altogether. You can have all the “safe harbors” and well-meaning privacy laws you want. But without enforcement and penalty, and without right of private action and access to efficacious and assertive legal advocacy that doesn’t bankrupt you until you give up, all this “safe harbor” talk is just illusory.
PHPs Have No Clear Independence From MLBs – Not In Finances, In Mission, Or In Professional Boundaries.
Not In Finances:
PHPs may be exclusively (curiously so) contracted in each state as the sole providers of these specialized services and which are supported in significant part by MLBs.
Let’s just pause for a moment and ponder this: an entity - a state medical board, holding itself out as a state agency or instrumentality operating with a wall of immunity, is yearly giving sizable grants, at that from fees it’s collected from licensees, to an exclusively contracted group of diverse non-physician counselors operating as a 501c3 educational entity that is conducting diagnostic psychiatric evaluations under the deceptive cover of “peer review,” doing so without a corporate medical license or malpractice insurance, denying the licensee access to their own diagnostic assessment report, while also claiming to not just the state auditor but to US DHHS and all physician clients that it does not do diagnostic evaluations and thus is not subject to HIPAA’s confidentiality protections and right of record access. But meanwhile these evaluations, conducted in complete denial of due process, serve as the basis to publicly declare a physician mentally ill, substance-abusing, disruptive, and a danger to society and thus warrant immediate revocation of their license via that board’s state-granted emergency police powers. Do you hear any alarm bells going off, or is this just my PHP-diagnosed mental illness kicking up again?
Not In Mission:
PHPs’ relationship with boards is not distinct and their joint missions to “protect the public” is certainly curious.
PHPs used to have as their mission the rehabilitation of the physician. How did “protecting the public” become so prominent? Can anyone tell me out of a sample of a thousand PHP evaluations of physicians, how many pertain to “protecting the public” from this dangerous physician? This is not only a ruse, enrobing themselves in some heroic role, it’s an affront to all who seek their services. Thus, with this ethic, anyone who traverses their door will automatically be seen as a threat to public safety. Does this not introduce some element of, shall we say, bias into the assessment process?
And you wonder why physicians are a tad hesitant to “get help?”
Perhaps for this noxious reason alone, the PHP system as currently deployed should be promptly funneled to a trash bin, but not before it is held accountable for the harms it has caused.
One does wonder why PHPs have chosen to make their mission indistinguishable from MLBs’. Could it be they need to solidify their immunity?
Not In Professional Boundaries:
MLB members may also sit on PHPs’ boards of directors (remember, they’re “educational non-profit organizations”) as well as occupy leadership positions in medical societies. And they rotate amongst them like three interacting merry-go-rounds, one jumping into the newly vacated slot of another who’s doing a synchronized jump to the next interconnected board. It’s the corporate equivalent of inter-family incest. It certainly doesn’t indicate independence of function. It’s just the same pool of ideological clones giving the public the appearance of diversity and fresh thinking. One gets the sense that they were specially chosen for their affable ethic of “going along to get along.” I suspect not one of them has the psychological makeup requisite of a whistleblower, namely the daringness of not going along and facing the consequences of not getting along.
PHPs’ Professional Training Is Obscure.
There Is No Indication That PHP Staff Are Truly Trained To Deal With These Unique Worklife Stress Issues, Especially As Few Are Physicians.
In fact, you will be hard-pressed to determine any training criteria for PHPs or, for that matter, even licensing requirements.
How is that possible? you might ask. Because it seems, PHPs are desperate to avoid identification as “clinically diagnosing entities” which would make them subject to malpractice liability – and to HIPAA which mandates prompt access to one’s medical record and ensures protection of the privacy of one’s PHI. Most carry no medical malpractice insurance; some have no physician on staff at all! How they are able to psychiatrically and medically evaluate referrals to their “preferred centers” remains a mystery. How are they able to conduct diagnostic lab tests and validly interpret them without medical training? Again, should there be concerns here?
Apparently, you don’t need a medical license to conduct a life-altering diagnostic assessment and send someone to the career death chamber. Joey the 7-11 cashier and Vinnie the plumber who are buddies in AA can open shop as a PHP. Making a diagnosis is a cinch - just say they all have alcoholism, are in denial, and are a danger to society. Back it up with false-positive tests and send them to your “preferred center” in Kansas for confirmation. Ka-ching! They balk? Tell your people at the board they’re bad news and let the board out them as town drunks and a danger to society. Done deal. No more problem. Next?
PHPs’ origin having likely been benevolent in creating a rehabilitative diversion program for alcoholic docs, their predominant focus of late has been routing people into “preferred” 4-day out-of-state “assessment programs” and from there 3 month stays in special cash-on-the-barrel, pre-paid “impairment programs for physicians,” permanently labeling their rehabilitatees as drunks, druggies or dangerously mentally ill and sentencing them from there to five years of “monitoring” and drug testing weekly, of course using that state PHP’s exclusively contracted “preferred” lab.
PHPs Apparently Receive No Training In Health Law, Regulatory Or Corporate Compliance Law, Or In Medical Ethics.
It appears that, like MLBs, they receive utterly no training in law or ethics. Such principles as due process, patients’ rights, the privacy of PHI, disability, ethical sensibility (!) … it appears that these are foreign concepts that reference esoteric laws and principles that have nothing to do with them.
No Oversight Or Accountability.
Further, they have utterly no incentive to become educated in these matters as, hey, there’s no oversight and no medico-legal accountability. They operate as independent fiefdoms within the state.
As awful as this is (truly, it’s enough to drive one to insanity just continuing to read it; I know, because it’s enough to drive me over the edge writing it), a definitive antidote that could bring these abuses to an immediate halt is instituting thoroughly independent oversight, medicolegal accountability, and assuring due process throughout. But, as will be seen below, there’s a curious resistance to this.
Currently, PHPs do not ensure “medical due process” of their diagnostic evaluations. I term it “medical due process” as due process is a concept applicable only to the legal arena. There is no such concept in medical evaluation and treatment. The closest thing comparable is patients’ rights. But because PHPs eschew a medical identity, they ~ thus far ~ have evaded accountability as either HIPAA or 42 CFR Part 2 entitles - their evaluees are not “patients.” My personal opinion is that they operate so deceptively as to invoke the FTC Act. But, let me remind the reader, I am not a lawyer. But if I were, this is one heavy-duty piece of legal machinery I’d bring to court.
It appears that PHPs generally operate with neither external nor internal oversight. That’s correct. None. And yet completely ignoring federal and state laws regarding PHI privacy, patients’ rights, and understandings of “regarded as disabled” protections under ADA, they enjoy some ever-elusive element of state immunity and are thus immune from suit. Their carefree attitude in valiantly “protecting the public” in this rights-abusive way seems to be “so, sue me Doc, ha ha ha ha ha …. Besides, who’s the public and the courts gonna believe, us, or you, a mentally ill drunk? Ha ha ha ha …. It doesn’t matter that it’s not true … that’s for you to prove. Ha ha ha ha ha ….”
As a result of the complete lack of oversight and accountability, some, perhaps all, of these PHPs have been using urine alcohol tests that are known to produce false positives and were most strongly and repeatedly advised against in this setting by SAMHSA.10 But since boards and the courts are wholly ignorant of these impermissible uses, PHPs continue to use them.
MLBs have been informed about this deceit as have national medical and psychiatric societies, US Attorneys, US DHHS OCR, US DOJ, state Attorneys General and Governors. All – ALL – have turned a deaf ear. “Whatever you need to do to get an impaired doc out of practice, whatever way you define it or even find it out, fine with us, just do it” seems to be the complicit endorsement.
While The Concept Of A Wellness Program Is Surely Good, As We All Know, ‘Free’ Usually Comes With A Cost.
So, who’s paying? What interests do they have? What protection of your utmost private medical information, your psychological health, is afforded you? And what recourse do you have in the event of a violation?
It will be vital to track the money of who is paying for these newly emergent “wellness programs.” If it’s the same responsibility-avoidant medical societies that spawned the PHPs, perhaps you best politely decline the outreach.
While state medical societies often proudly exclaim that they are the originators of their PHPs, they refuse to take ownership of their harms.
What Is A Safe Harbor “Wellness Program?” Who Approves Such Designation?
What anyway is a safe harbor “wellness program?” Who approves its entrance into the service arena as an “authorized program?”
Pardon if I ask the obvious but “what IS a Wellness Program?” And perhaps even more to the point, how is a “wellness program” different from an “illness program?” If an “illness program” assesses, i.e. diagnoses, and treats illness, what’s a “wellness program” do? Fine and dandy if you say it assesses your state of wellness and offers prescriptives - even scientifically based ones - that shore up wellness. But what if in assessing your wellness, it says “uh oh, you’re not so well, doc; in fact, you’re ill. You have {pick any: burnout; depression; substance use disorder; PTSD; moral injury; PITA syndrome …]” and they offer to treat you, all within the bounds of their professional licensure and training. Are they still a “wellness program?” If I’m the client who went there with burnout and depression and grief from too much trauma, is my treatment still covered under this safe harbor “Wellness Program” designation?
Is An Individual Therapist A Safe Harbor “Wellness Program?”
And … is an individual therapist or a psychiatrist a “wellness program?” What if the licensee physician has in fact developed bona fide disabling depression, i.e. “impairing,” and is started on meds or perhaps even needs to be hospitalized? Are they still assured of such protection? What if they’ve reported in this session that they’ve increased their use of alcohol or that they smoke pot to relax? Can that be reported to a MLB or “impairment committee” from a “wellness program?” (Oh, sorry Charlie, that’s not covered. Off you go to Kansas….)
What about many states’ overly expansive mandatory reporting of “suspicion of impairment?” Is the doc still safe if they’re in one of these wellness programs and someone makes such an allegation? Who talks to whom?
What if a physician had a preexisting condition such as a prior post-partum depression? What if a physician had anxiety or depression, not per se related to physicianhood but, say, to a deteriorating marriage or other major life stresses? Are they safe in such a program?
Who I wonder is advising legislators on considering these complexities?
Who defines the core criteria for such a “Wellness Program?” On what model is it based?
I fear that without such careful consideration, the well-intentioned programs may turn out to not really be safe harbor “Wellness Programs” but in fact could subtly morph into some new-agey rebranding of PHPs behind yet another facade of benevolence and safety.
But We’re Talking About A Whole New Start – Wellness Programs – You Sourpuss …. So Why This Anti-PHP Tirade?
So why do I go on this tirade about PHPs when this is supposed to be about the good “wellness programs” that are being endorsed?
Because without naming these abuses and without specifically warning that these same PHPs may now don the seductive costume of “physician wellness” prancing about empathizing so meaningfully about physicians’ burnout plight, the same harms will ensue, this time under an even more devious “wellness” camouflage.
But here’s especially why. Because, raw truth be told, physicians can’t risk getting screwed again. And as anyone who’s been multiply screwed knows, you have a very limited psychological quota for that kind of betrayal.
Burned Out, Traumatized, And Morally Injured, Physicians’ Psychological Resiliency Is Stretched Thin. There Is No Leeway For Additional Betrayal.
Thus, the main good I see coming from these presumptively well-intentioned legislative initiatives is that when physicians do go for psychologically-oriented help, and if and only if they seek such help from a “program” specifically designated by someone under some authority as a “wellness program” under this safe harbor type legislation, they may - may - get such help with all the force of ... the promise of … assured confidentiality.
But … do the bills/laws have real teeth? And what are the penalties for not abiding by such sacrosanct confidentiality? Without such accountability, these laws are little more than “suggestions.” The law governing peeer review – the Health Care Quality Improvement Act – looks wonderful on paper. It’s toothless when it comes to enforcing physicians’ rights against hostile and permanently maiming sham peer review. Wanna see proof?11
So Many Questions Remain Unanswered.
And given so many MLB, PHP, and medical societies’ hands in such legislation without hearing (in fact overtly avoiding) the voices of those who know how these powers have crushed physicians behind the veneer of therapeutic benevolence and the ever-heroic banner of “protecting society,” I would encourage extreme caution in approaching ANY physician health or wellness program until open, public discussion of these abundant concerns has been had.
My Suggestions …
What’s really needed is a no-questions-asked “Wellness Health Insurance Benefit” for physicians seeking care. Pay for it out of licensing fees. (After all, that’s how PHPs are supported.) Ten or twenty sessions. No diagnosis needed. Covered! Physicians choose who they see. And that would include appropriately trained physician coaches who know the difference between wellness and illness. If a diagnosis needs to be made for treatment purposes, then arrange a different mental health benefits program while still protecting to the utmost the absolute confidentiality of the sessions and the treatment record. And hold all therapists and psychiatrists and coaches accountable via signed contract specifying penalties for unauthorized disclosure. It must be iron-clad sacrosanct.
In All Circumstances, Get The Help You Need.
My advice to docs, PGYs, and med students: approach these new “wellness programs” with openness to exploration but “eyes-wide-open” caution. Meanwhile, get the help you need from a private entity whose confidentiality you can rely on and who has sufficient expertise in the areas that physicians are grappling with, e.g. high-intensity stress and psychological trauma; PTSD, and moral injury. Get referrals from trusted sources. Get their assurance that they abide by prevailing rules of beneficence and confidentiality. And insist that, unless a clear major mental illness is felt to be present, no diagnosis be entered in the record.
Will you have to pay out of pocket - likely.
Will you be safe from disclosure - in all likelihood yes.
In all circumstances, get the help you need.
Fellow physicians, I write this out of deepest respect and heartfelt concern. You are an invaluable resource. You have devoted a significant part of your adult life to have the right to practice this time-honored profession in the service of mankind. And you have a right to obtain the mental health services you need without fear of ostracization, bankrupting four-day out-of-state evaluations, or career homicide.
You have a right to leave work for such treatment under FMLA. If boards or credentialing entities ask impermissible questions regarding your diagnosis or treatment or even the fact of your seeking help, respectfully question in writing their authority to ask such under ADA. Failing their response, consider filing a complaint with the US DOJ CRD or other respective agency. If they threaten or take retaliation, get an informed employment lawyer savvy in ADA and health law. Retaliation is prohibited under HIPAA, 42 CFR Part 2, ADA, FMLA (and others) and is punishable with civil penalty.
And meanwhile, let’s join forces to hold MLBs and PHPs accountable for upholding laws that protect physicians’ rights to access needed psychological and medical care without recrimination and to be held fully legally accountable for ensuring the non-interference with receipt of such necessary safe care.
Above all, please take good care of yourself, and let’s take good care of each other.
* * *
Two disclaimers and an invitation:
1) The author is not a lawyer though probably should’ve been. Just so that you know my orientation and determined persistence, my guru would be Brig. Gen. Telford Taylor, Chief Prosecutor of Nazi war crimes at Nuremberg. His Opening Statement in the Doctors Trial is as passionate as one will ever see in law. He’s considered to be the visionary founder of international law. Want an inspiring read?, this piece is sheer eloquence (… shorter than this relentlessly growling post, btw).
2) The admittedly strong opinions and at times bitterly cynical descriptors within are this author’s alone and are not meant to encompass others as co-responsible fire-breathers. I so wish I could write about a benevolent, well-received, model PHP. Unaware of such and absent any productive dialog with NCMB, NCPHP, FSPHP or FSMB, I’m left with few options other than creative linguistic exercises in acid etching on paper.
My invitation: Whether you find emphatic YES! agreement and heartening reassurance in these words, or they invoke vein-swelling, scream-hoarsening rage, I’d welcome your comments below - appropriately modulated of course, and also your widely sharing on all available vehicles - social media and paywalled private organizations as well. After all, the MRTC people get to publish pro-PHP pieces in deeply important and silently influential vehicles like the Judges Journal which serve to subtly influence the court system’s assent to the “PHP Blueprint” model which essentially rationalizes violation of multiple federal laws via fundamentally flawed and oft-repeated scientific studies.12 I again extend an offer to have a public dialog about these matters with interested persons especially from FSMB and FSPHP and its various state members. I know I could gather quite the crowd to explore DuPont and Merlo’s PHP Blueprint and its incestuous self-exultory progeny.
Lastly, to wash your brain free of this tirade, take a few slow deep breaths and relish this beauty. It’s a picture of a truly safe harbor that I took on my walk yesterday evening. Eastern Point, Entrance to Gloucester Harbor. What a joy to be here! And what a joy it would be for every physician to truly enjoy safe harbor.

Generally when a law is enacted and you’re told that it will benefit you, you take it on faith and gloss over it, as laws are written in their customarily obscure and soporific ways. But on closer read, you discover that not only is the new law not helpful in the ways propounded but it’s actually problematic and could be detrimental.
For example, in NC, NCPHP’s 2014 performance audit by the NC auditor revealed, in essence, they had violated the due process rights of 1,140 physicians over the preceding decade (operating deceptively as a “peer review” organization) by declining to provide them with their diagnostic evaluations and refusing to allow them to contest their diagnostic assessment and provide an independent professional opinion. After I complained vigorously that what NCPHP conducted in no way resembled “peer review” as it portrayed to the auditor it had conducted, powers presumably representing the board, PHP, and possibly the medical society substantially revised NCGS 90, The Medical Practice Act – the law governing the board and PHP. They simply up and removed reference to NCPHP conducting peer review - zap gone! - alas, along with its requisite provision of due process. The revised law newly gave the NCPHP group medical diagnostic powers, despite its not being licensed as a medical corporation, and did so with no staffing or training requirements, while at the same time removing reference to guaranteeing due process or its medical equivalent. It further used idiosyncratic language that conceivably could still jeopardize most physicians who are subjected to its now permitted invasive forensic diagnostic psychiatric evaluations. But even more circumspect, the drafters of this law made it clear they wanted no input from anyone outside of their circle - well, at least not mine. Sadly, it remains seriously defective law which will be manifest when the next physician tries to assert his/her rights.
PHP - Physician Health Program
MLB - Medical Licensing Board
MRTC - the Medical Regulatory Therapeutic Complex
FSMB - Federation of State Medical Boards
FSPHP - Federation of State Physician Health Programs
ADA - The Americans with Disabilities Act
HIPAA - The Health Insurance Portability and Accountability Act
HITECH Act - The Health Information Technology for Economic and Clinical Health Act
42 CFR Part 2 - Confidentiality Of Substance Use Disorder Patient Records
PHI - Protected Health Information
SAMHSA - The Substance Abuse Mental Health Services Administration
FMLA - Family Medical Leave Act
US DHHS - OCR - US Department of Health and Human Services (regulates, along with state Attorneys General, HIPAA enforcement); OCR - Office of Civil Rights
US DOJ CRD - US Department of Justice Civil Rights Division
Medical Regulatory Therapeutic Complex. See “Systematic Abuse and Misuse of Psychiatry in the Medical Regulatory-Therapeutic Complex” (link: https://www.physicianrights.net/articles)
If you happen to have been at that FSMB presentation or accessed its slide handout made available for more than 18 months, I’d welcome hearing from you.
So, in Florida, your choice appears to be: go for the PHP brain biopsy and be forever ostracized as iatrogeically brain-damaged; or, resist and be cast out of medicine as an allegedly dangerous mentally ill, drug abusing former doc on the run. Either way, you’ll be fortunate to secure employment at Walmart.)
It recently updated these guidelines, though curiously behind a paywall. Here’s the earlier one from 2011: https://www.fsmb.org/siteassets/advocacy/policies/physician-impairment.pdf
To quote Dr. Warren Pendergast, formerly Medical Director of NCPHP and FSPHP’s president: “One reason for this discrepancy [alleged better outcomes for physicians] may be physician assistants as a group don’t have the same ability to pay for long-term treat- ment. ‘They just don’t have as deep of pockets as the physicians when they get into trouble,’ say Warren Pendergast, M.D., medical director of the North Carolina PHP and coauthor of the study. Another contributing factor may be that physicians have more to lose. ‘For a lot of physicians, if they’re not able to keep their license or get their license back, they don’t have a lot to fall back on,’ says Pendergast. ‘Many of us don’t have other skills. Medicine is really all we’ve done.’ The prospect of losing one’s livelihood and identity as a physician is a major motivator.” Journal of Medical Licensure and Discipline. Vol 91, Number 4. 2005 (Page 8).
Ironically, the good side of this would be some element of federal protection of fairness and due process and an appeals process woven throughout with checks and balances protecting all parties’ interests and rights. That is, in a world where this was reliable behavior on the part of a government. Alas, we’re still navigating our way through upside-down.
See “Professional Practice Guidelines for Occupationally Mandated Psychological Evaluations” http://www.apa.org/practice/guidelines/psychological-evaluations.aspx
See: The Role of Biomarkers in the Treatment of Alcohol Use Disorders, 2012 Revision. Spring 2012, Volume 11, Issue 2. Curiously, I can no longer find it on SAMHSA’s site.
See: Dr. Lawrence Huntoon - Sham Peer Review Archive – https://aapsonline.org/sprarchive/
See “Physician Health Programs: A Model for Treating Substance Use Disorders” from the winter 2018 issue of The Judges’ Journal, authors Robert L. DuPont and Lisa J. Merlo.