


New Safe Harbor “Wellness Programs” To Protect Physicians in Getting Help (The SHORTY Version)
Maybe not so safe ... Maybe only if you're 100% certifiably "well"

(This is the SHORT version of a considerably lengthier article of the same title. The longer version has abundant references and explanatory excursions. Here’s a link to it.)
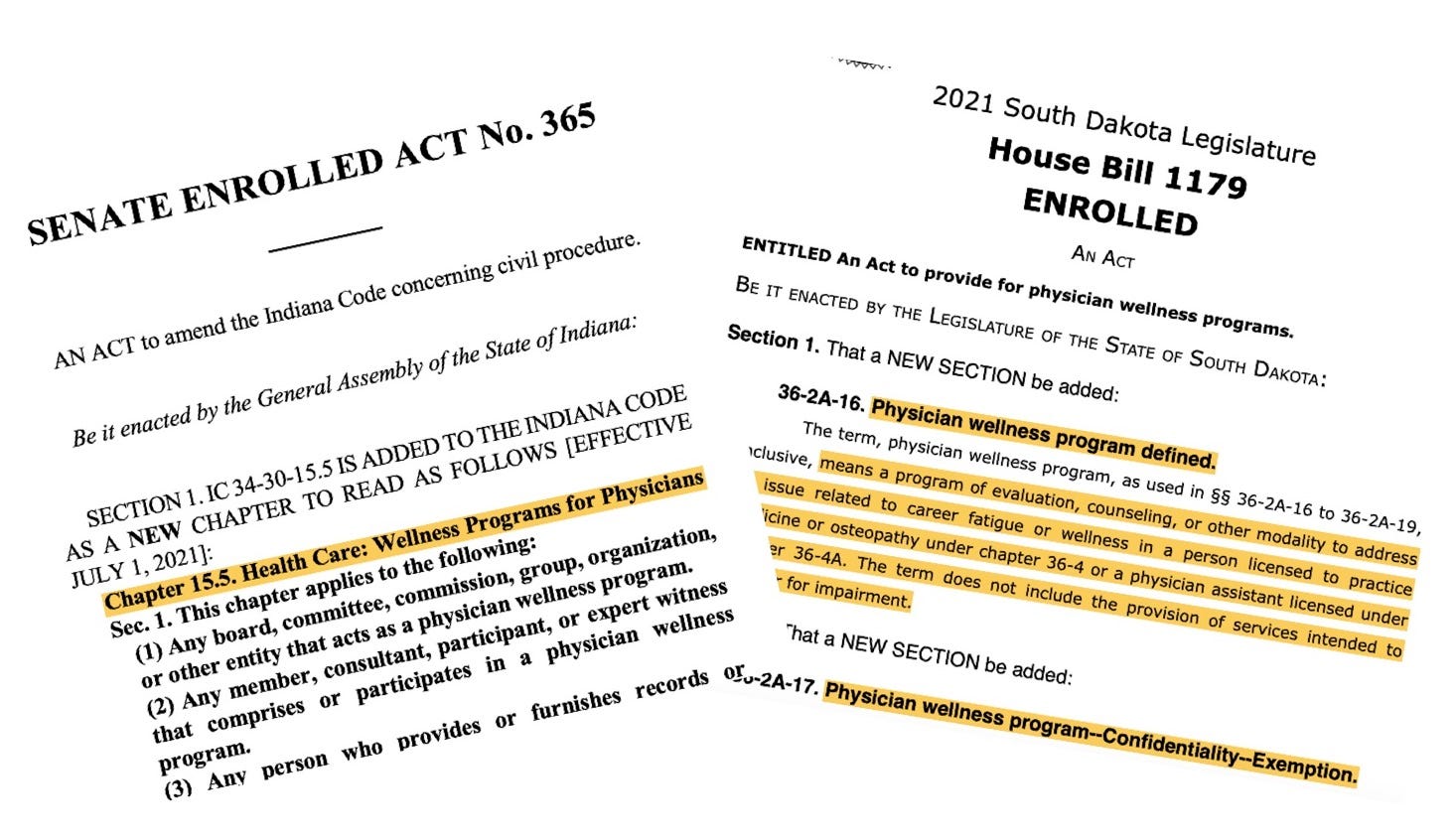
Recent bills and enacted laws in three states are designed specifically to protect confidentiality for physicians seeking help for psychologically oriented “wellness services” in the context of their professional lives. (You may have thought that your confidentiality was already protected. You would have been mistaken.)
While on the surface there appears to be cause to be reservedly enthusiastic and hopeful, I’ve got numerous - and growing - reservations. I still see significant danger for physicians who seek any such services from these newly-minted wellness programs, especially if they’re operated by any party affiliated in any way with boards or PHPs. I maintain grave concerns about the ever-evasive, chameleon-like identity of PHPs and their boundariless fluidity with boards (MLBs).
Of the three states, South Dakota’s and Indiana’s appear most straightforward and indeed secure. I can’t make heads or tails of Virginia’s. Which, by the way, is one of the problems with this sort of legislation. If you, a reasonably intelligent professional, can’t make sense of it, you can be certain of one thing: you don’t have a solid footing to protect your rights.
See footnote below for some abbreviations you may see peppered throughout. 1
The Newly Legislated “Wellness Programs”
First, The Good News. Why I Believe These Bills/Laws (At Least Two Of The Three) Are Helpful. It’s Not Per Se In What They Propose As Much As In What They Signify.
They demonstrate legislators’ genuine concern about physicians’ not being able to safely get psychological help without being pulled into the board’s and PHP’s crazy-making universe and being driven to either suicide or bankruptcy and a life of morally assaulted despondency. These legislative efforts give formal recognition that docs as a whole are in trouble with burnout, the toll of trauma and PTSD, and deep moral injury. And they need exquisitely skillful help that is focused, effective, readily available, and air-tight fail-safe to obtain. Are these “wellness” services? Well, if you call a medic’s stemming life-threatening hemorrhage of a soldier’s traumatic injury a “wellness service,” okay.
So, in a very indirect, non-accusatory way, these new laws recognize that getting help through a PHP may be dangerous for physicians’ careers and their personal wellbeing. But these bills tiptoe around the predatory culprits which have made safely getting help impossible.
They also recognize that such help needs to be safe from medical boards’ prying eyes and their assaultive police power overreach. They seem also to recognize that getting psychological help in any way is dangerous as, if you have to report it to an entity such as a board or a credentialing entity for your staff appointment and your employment, it could irreparably harm you as it could suck you into the MRTC vortex from which you have little chance of escape or career survival.
Why These Wellness Program Bills/Laws May Be Inadequate If Not Dangerous.
First, they generally legitimize PHPs as the widely accepted deliverer of both physician impairment and now of psychological wellness services. And there’s no basis in fact for affirming either except for PHPs’ relentless self-affirmations that they are the definitive go-to authority. Sorry to differ. They aren’t.
By legislators giving such tacit approval, they still feed docs into a dangerous PHP system with its “preferred relationships” that more resembles a self-interested referral scheme if not a RICO, and perpetuates its lack of definitional and thus legal-delimiting boundaries. They don’t recognize PHPs’ inherent lack of independence from MLBs. And they still make no effort to hold PHPs and MLBs accountable for their past denial of rights.
No accounting for past harms
These bills indirectly give deference to PHPs as the wellness program deliverers.
But many contend these very physician health programs perpetuated the harms that drove the production of these new “safe harbor wellness program” laws. These bills/laws do not account for past harms by these invasive boards and PHPs which have punished – via “medicalization,” indeed “extraordinary rendition” – physicians who have sought help in contexts that were entirely outside of any patient complaint or quality of practice concern. To me, ignoring these harms is like telling Jack the Ripper that he can continue to date as long as we don’t hear another peep (or scream).
PHPs operate as chameleons under diverse and continuously changing deceptive identities that then become ensconced in state law and give them protection. Witness this sampling: “peer review;” “case manager;” “screening program;” “facilitator of referral to a ‘preferred program’” etc.
PHPs are generally not licensed as medical corporations and yet are conducting life-altering diagnostic evaluations (or “screenings”) whose results they refuse to share with physicians but which results they disclose to boards which then order unquestioning compliance with whatever the PHP says, presumably including brain biopsy if they so chose. (I write this in only slight jest; visit FL laws to see what a PHP can do, non-compliance with which will essentially cast you out of medicine worldwide as a pariah to be scorned.)
From my perspective, there is no imaginable scenario in which a physician should ever willingly initiate going to a PHP.
PHPs’ Mission Creep
The PHP movement has been expanding its scope of declared expertise. That it actually possesses the declared expertise is highly suspect.
There’s a movement afoot by PHPs to classify burnout as depression. Now, with depression as a “mental illness” and all of its stigma, depression is now thus a “danger to patient safety.” So now, you’re not just burned out. You’re mentally ill and a danger to society!
Further, everyone who walks through the PHP door is by definition “impaired.” Otherwise, they reason, “why would you be sent comrade?” To FSMB, there is no distinction between actual functional work impairment from a bona fide disability, a physician’s “potential for impairment,” and anyone having a medical condition that is “potentially impairing.” When simply living and practicing your profession is a risk factor for being alleged to be “potentially impaired” and thus a danger to patient safety, you’ve got a problem.
Once ensnared, no matter how warrantless or mistaken, that physician’s career is over. And due to boards’ and PHPs’ wall of immunity, maintained somehow with utterly no governmental oversight, no justice or monetary recovery is available. You’ll be hard-pressed even to find a sufficiently expert lawyer conversant in this area. The bottom line here is, once pulled into their twilight zone, your career, your life as you once knew it, is over.
And there will be no - NO - intervention by the state because the state has chosen not to see either its board or its contracted PHP as a possible manipulative wrongdoer capitalizing on its immune status. It’s much easier to let them “discipline their own” and step back. Because surely, no one wants an “impaired physician.” So let them do whatever they need to do.
PHPs Have No Clear Independence From MLBs – Not In Finances, In Mission, Or In Professional Boundaries.
Not in finances:
PHPs may be exclusively (curiously so) contracted as the sole providers of these specialized services and supported in significant part by MLBs.
Not in mission:
PHPs’ relationship with boards is not distinct and their joint missions to “protect the public” is certainly curious.
PHPs used to have as their mission the rehabilitation of the physician. How did “protecting the public” become so prominent? This is not only a ruse, enrobing themselves in some heroic role, it’s an affront to all who seek their services. Thus, with this ethic, anyone who traverses their door will automatically be seen as a threat to public safety. Does this not introduce some element of, shall we say, bias into the assessment process?
Perhaps for this noxious reason alone, the PHP system should be promptly funneled to a trash bin.
Not in professional boundaries:
MLB members may also sit on PHPs’ boards of directors (remember, they’re “educational non-profit organizations”) as well as occupy leadership positions in medical societies. And they rotate amongst them like three interacting merry-go-rounds, one jumping into the newly vacated slot of another who’s doing a synchronized jump to the next interconnected board. It’s the corporate equivalent of inter-family incest. It certainly doesn’t indicate independence of function.
PHPs’ Professional Training Is Obscure.
There is no indication that PHP staff are truly trained to deal with these unique worklife stress issues.
In fact, you will be hard-pressed to determine any training criteria for PHPs or, for that matter, MLBs.
How is that possible, you might ask. Because it seems, PHPs are desperate to avoid identification as “clinically diagnosing entities” which would make them subject to malpractice liability - and to HIPAA.
PHPs apparently receive no training in health law, regulatory or corporate compliance law, or in medical ethics. Such principles as due process, patients’ rights, the privacy of PHI, disability, ethical sensibility (!) … it appears that these are foreign concepts that reference esoteric laws and principles that have nothing to do with them.
No Oversight Or Accountability.
Further, they have utterly no incentive to become educated in these matters as, hey, there’s no oversight and no medico-legal accountability. They operate as independent fiefdoms within the state.
Currently, PHPs do not ensure “medical due process” of their diagnostic evaluations. I term it “medical due process” as due process is a concept applicable only to the legal arena. There is no such concept in medical evaluation and treatment. The closest thing comparable is patients’ rights. But because PHPs eschew a medical identity, they ~ thus far ~ have evaded accountability as either HIPAA or 42 CFR Part 2 entitles. My personal opinion is that they operate so deceptively as to invoke the FTC Act.
Completely ignoring federal and state laws regarding PHI privacy, patients’ rights, and understandings of “regarded as disabled” protections under ADA, they enjoy some ever-elusive element of state immunity and are thus immune from suit. Their carefree attitude in valiantly protecting the public in this rights-abusive way seems to be “so, sue me Doc, ha ha ha ha ha …. Besides, who’s the public and the courts gonna believe, us, or you, a mentally ill drunk? Ha ha ha ha …. It doesn’t matter that it’s not true … that’s for you to prove. Ha ha ha ha ha ….”
While The Concept Of A Wellness Program Is Surely Good, As We All Know, ‘Free’ Usually Comes With A Cost.
So, who’s paying? What interests do they have? What protection of your utmost private medical information is afforded you? And what recourse do you have in the event of a violation? What anyway is a safe harbor “wellness program?” Who approves?
But … is an individual therapist or a psychiatrist a “wellness program?” What if the licensee physician has in fact developed bona fide disabling depression and is started on meds? Are they still assured of such protection? What if they’ve reported in this session that they’ve increased their use of alcohol or that they smoke pot to relax? Can that be reported to a MLB or “impairment committee” from a “wellness program?” What if a physician had a preexisting condition such as depression? What if a physician had anxiety or depression not per se related to physicianhood but, say, to a deteriorating marriage or other major life stresses? Are they safe in such a program?
Without such careful consideration, the programs are not really safe harbor “Wellness Programs” but are some new-agey rebranding of PHPs behind yet another facade of benevolence and safety.
The Beguiling Apparition Of Law-Guaranteed Privacy
Despite intensive study over the past six months of HIPAA, HITECH, 42 CFR Part 2, ADA, diverse state privacy laws, laws governing the medical evaluation of employees et al., I still remain uncertain about what parameters apply to PHPs regarding privacy of PHI obtained from their impermissible interrogations. Even more vague the federal and state privacy laws protecting such “wellness programs.” Are they covered under HIPAA, 4 CFR Part 2, and any other federal or state laws?
You can have all the “safe harbors” and well-meaning privacy laws you want. But without enforcement and penalty, and without right of private action and access to efficacious and assertive legal advocacy that doesn’t bankrupt you until you give up, all this “safe harbor” talk is just illusory.
But We’re Talking About A Whole New Start – Wellness Programs …. So Why This Anti-PHP Tirade?
So why do I go on this tirade about PHPs when this is supposed to be about the good “wellness programs” that are being endorsed? Because without naming these abuses and without specifically warning that these same PHPs may now don the costume of “physician wellness” prancing about empathizing so meaningfully about physicians’ burnout plight, the same harms will ensue, this time under an even more devious “wellness” camouflage. And, truth be told, physicians can’t risk getting screwed again. And as anyone who’s been multiply screwed knows, you have a very limited psychic quota for that kind of betrayal.
Burned out, traumatized, and morally injured, physicians’ psychological resiliency is stretched thin. They is very limited leeway for additional betrayal.
Thus, the main good I see coming from these presumptively well-intentioned legislative initiatives is that when physicians do go for psychologically-oriented help, and if and only if they seek such help from a “program” specifically designated as a “wellness program” under this safe harbor type legislation, they may - may - get such help with promised assurance of confidentiality.
But … do the bills/laws have real teeth? And what are the penalties for not abiding by such sacrosanct confidentiality? Without such accountability, these laws are little more than “suggestions.”
Too Many Questions Remain Unanswered.
And given so many MLB, PHP, and medical societies’ hands in such legislation without hearing (in fact overtly avoiding) the voices of those who know how these powers have crushed physicians behind the veneer of benevolence and the ever heroic banner of “protecting society,” I would encourage extreme caution in approaching ANY physician health or wellness program until open, public discussion of these abundant concerns has been had.
My Suggestions …
What’s really needed is “no questions asked” Wellness health insurance benefits for physicians seeking care. Ten or twenty sessions. Covered. Physicians choose who they see. If a diagnosis needs to be made for treatment purposes, then arrange a different mental health benefits program while still protecting to the utmost the absolute confidentiality of the sessions and the treatment record. And hold all therapists and psychiatrists accountable via signed contract specifying penalties for unauthorized disclosure. It must be iron-clad sacrosanct.
In All Circumstances, Get The Help You Need.
My advice to docs, PGYs, and med students: approach these new “wellness programs” with “eyes-wide-open” caution. Meanwhile, get the help you need from a private entity whose confidentiality you can rely on and who has sufficient expertise in the areas that physicians are grappling with, e.g. high-intensity stress and psychological trauma; PTSD, and moral injury. Get referrals from trusted sources. And insist that, unless a clear major mental illness is felt to be present, no diagnosis be entered in the record.
Will you have to pay out of pocket - likely.
Will you be safe from disclosure - in all likelihood yes.
But in all circumstances, get the help you need.
You are an invaluable resource. You have devoted a significant part of your adult life to have the right to practice this profession in the service of mankind. And you have a right to obtain the services you need without fear of ostracization or career homicide.
You have a right to leave work for such treatment under FMLA. If boards or credentialing entities ask impermissible questions regarding your diagnosis or treatment or even the fact of your seeking help, question in writing their authority to ask such under ADA. Failing their response, file a complaint with the US DOJ CRD.
And meanwhile, let’s join forces to hold MLBs and PHPs accountable for upholding laws that protect physicians’ rights to access care without recrimination and to be held fully legally accountable for the provision of such safe care.
P.S. This is what a safe harbor looks and feels like (Eastern Point, Gloucester MA, a ten minute walk from my house):

PHP - Physician Health Program
MLB - Medical Licensing Board
MRTC - the Medical Regulatory Therapeutic Complex
FSMB - Federation of State Medical Boards
FSPHP - Federation of State Physician Health Programs
ADA - The Americans with Disabilities Act
HIPAA - The Health Insurance Portability and Accountability Act
HITECH Act - The Health Information Technology for Economic and Clinical Health Act
42 CFR Part 2 - Confidentiality Of Substance Use Disorder Patient Records
PHI - Protected Health Information
SAMHSA - The Substance Abuse Mental Health Services Administration
FMLA - Family Medical Leave Act
US DHHS - OCR - US Department of Health and Human Services (regulates, along with state Attorneys General, HIPAA enforcement); OCR - Office of Civil Rights
US DOJ CRD - US Department of Justice Civil Rights Division